Why Retinol?
Retinoids (retinol, retinaldehyde, tretinoin) are some of the best‑studied topical ingredients for fine lines, uneven tone, rough texture and acne. They work by increasing epidermal turnover, stimulating collagen, and normalising keratinisation.¹–⁶
Please remember if you are pregnant of breastfeeding retinol is not advised
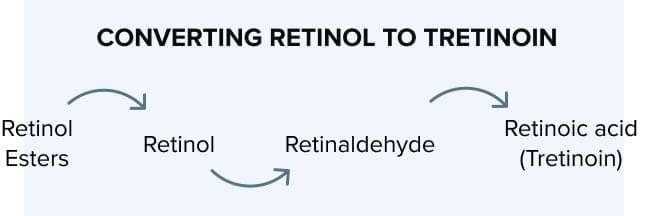
Retinol vs Retinaldehyde vs Tretinoin: What’s the Difference?
Retinol converts to retinaldehyde, then to all‑trans retinoic acid (tretinoin) in the skin; it’s effective, widely available, and generally better tolerated than prescription tretinoin.¹˒⁴
- Retinaldehyde (retinal) is one metabolic step away from retinoic acid, so it’s typically more potent than retinol yet still relatively well tolerated.²˒⁷
- Tretinoin (prescription retinoic acid) has the strongest evidence base for photoageing but is also the most irritating, so it’s best used with professional guidance.³–⁶

Retinol by Age
In Your 20s – Prevention & Glow
Best choice: 0.1–0.3% retinol or retinyl palmitate for gentle prevention.¹
- Why: Early, consistent use may help maintain collagen and even tone while minimising irritation.¹
- Frequency: Start 1–2 nights/week, increase as tolerated.¹˒⁴
Suggested Product:
Boots Ingredients Retinol Serum 0.3%
A basic, affordable 0.3% pure retinol serum (~£7) that’s great for introducing retinoids. Trusted high-street option, ideal for oily/combination skin. It follows the maximum retail OTC limit and reflects dermatologist advice to start low and slow.
In Your 30s – Smooth & Brighten
Best choice: 0.3–0.5% retinol or retinaldehyde for a potency bump with good tolerability.¹˒²
- Why: Fine lines and uneven pigmentation become more noticeable; mid‑strength over‑the‑counter retinoids often deliver visible improvements.¹˒²
- Frequency: 3–5 nights/week once tolerated.¹˒⁴
Suggested Product:
FaceTheory Retinal Supreme MultiCream (retinal)
Contains retinaldehyde, which converts faster to retinoic acid than retinol and is often better tolerated. Buffered with hydrating ingredients for dry/normal or sensitive skin. Best suited for stepping up potency in your 30s without over-irritation.
In Your 40s & Beyond – Repair, Firmness & Menopause Skin
Best choice: 0.5–1% retinol, retinaldehyde, or prescription tretinoin (with professional oversight).²–⁶
- Why: With falling oestrogen, collagen decreases and skin gets drier and thinner; stronger or prescription retinoids can better target firmness and lines—but tolerance must be managed carefully.⁸–¹¹
- Sensitive skin: Consider encapsulated/slow‑release retinol or alternate‑night use.¹˒⁴
- Resilient skin: Step up strength or frequency if well tolerated.¹˒³
Suggested Product:
Medik8 R‑Retinoate Intense (encapsulated high‑strength)
An advanced, encapsulated retinyl retinoate and retinaldehyde blend—8× more potent than standard retinol, as supported by brand’s clinical comparisons. Great for targeting deeper signs of ageing with better skin tolerance.** Recommended for resilient or well-acclimatised skin.
Retinol for Menopause & Perimenopause Skin
Collagen and dermal thickness fall with oestrogen decline, increasing dryness and sensitivity.⁸–¹¹
- Prioritise ceramides, peptides, urea, and fatty acids to support the barrier.
- Increase frequency before percentage to minimise irritation.¹˒⁴
- Consider retinaldehyde as a balance of efficacy and tolerability.²˒⁷
How to Start (Safely) – Evidence‑Aligned Best Practice
Patch test first (3–5 nights).¹˒⁴
- Apply a pea‑sized amount to dry skin; avoid immediate peri‑oral/eye areas until tolerant.¹˒⁴
- Buffering (“sandwich”): moisturiser → retinol → moisturiser for sensitive skin.¹˒⁴
- Titrate slowly: build nights per week first, then consider strength.¹˒⁴
- Daily SPF 30–50: retinoids increase photosensitivity and are degraded by UV.¹˒⁴˒¹²
Common Questions (FAQs)
Is retinol safe during pregnancy or breastfeeding?
Topical retinoids are typically avoided; seek personalised medical advice.¹³
Which is stronger: retinol or retinaldehyde?
Retinaldehyde is generally stronger (one step from retinoic acid) and can deliver faster results with comparable tolerability in studies.²˒⁷
What if I get peeling or redness?
Reduce frequency, buffer with moisturiser, or step down strength—then titrate back up cautiously.¹˒⁴
Can I combine vitamin C and retinol?
Yes—vitamin C in the morning, retinoid at night is a commonly recommended, well‑tolerated approach.¹˒⁴
Ready for a Personalised Retinoid Plan?
Not sure which molecule, strength or frequency is right for you?
Book your Retinoid Review Consultation with Skin Harmony Surrey. I’ll tailor a plan that fits your skin type, age, and tolerance.
References
Kafi R, et al. Improvement of naturally aged skin with vitamin A (retinol). Arch Dermatol. 2007;143(5):606‑612.
Creidi P, et al. Topical retinaldehyde on photoaged skin: a randomized, clinical trial. Dermatology. 1998;196(3):314‑317.
Olsen EA, et al. A double‑blind, vehicle‑controlled study of the effects of topical tretinoin on photodamaged facial skin. J Am Acad Dermatol. 1991;25(4):737‑745.
Mukherjee S, et al. Retinoids in the treatment of skin aging: an overview of clinical efficacy and safety. Clin Interv Aging. 2006;1(4):327‑348.
Griffiths CEM, et al. Restoration of collagen formation in photodamaged human skin by tretinoin (retinoic acid).N Engl J Med. 1993;329(8):530‑535.
Kang S, et al. Topical tretinoin (retinoic acid) improves photoaged skin. J Am Acad Dermatol. 1995;32(3):555‑559.
Sorg O, Saurat J‑H. Topical retinaldehyde, a natural precursor of retinoic acid, exerts retinoid effects with less irritation. Dermatology. 2014;229(3):183‑190.
Brincat M, et al. Long-term effects of the menopause and sex hormones on skin thickness. Br J Obstet Gynaecol. 1987;94(2):126‑129.
Affinito P, et al. Effects of postmenopausal hypoestrogenism on skin collagen. Maturitas. 1999;33(3):239‑247.
Sumino H, et al. Effect of aging and postmenopausal hypoestrogenism on skin elasticity and bone metabolism.Maturitas. 2004;48(2):97‑104.
Verdier‑Sévrain S, Bonté F. Skin hydration: a review on its molecular mechanisms. J Cosmet Dermatol. 2007;6(2):75‑82.
Niedner R, et al. Photostability of retinoids. J Am Acad Dermatol. 1990;23(3 Pt 1):523‑527.
Chien AL, et al. Safety of skin care products during pregnancy. Int J Womens Dermatol. 2018;4(4):168‑172.